Financial Policy Form
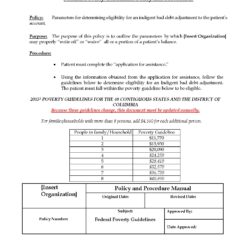
$20.00
*It is recommended that patients read and execute this agreement if they are unable to meet their entire financial obligation prior to being treated at your organization.
**It is also recommended that the patient or guarantor complete the credit card authorization for your organization.
***It is also recommended that when your organization makes a credit card charge or bank withdrawal that your billing department sends a receipt.